
CROI 2026: GLP-1 weight loss drugs include potential immune benefits in gut tissue
13 March 2026. Related: Conference reports, Weight, diabetes, metabolic complications, Coinfections and complications, CROI 33 (Retrovirus) 2026.

Simon Collins, HIV i-Base
CROI 2026 included an oral plenary talk on the use of GLP-1 receptor agonists in people living with HIV, plus an additional oral presentation and seven posters.
These covered the short-term impact of GLP-1s in a real-world setting, potential benefits on reducing smoking, cardiovascular risk, depression, and liver fibrosis, with an oral abstract on the potential to perhaps reverse the gut damage that occurs in very early HIV infection and that persists despite effective ART.
The excellent plenary overview by Todd Brown from Johns Hopkins University School of Medicine is recommended viewing for everyone, given the importance of this class of drugs and the impact they are having on healthcare – including with interrupted or discontinued use. The talk focused on the areas of strongest data and also highlighted significant gaps in the research that might have been missed or under appreciated in the rapid uptake and use of these drugs, also looking at their use in people of different ages. [1]
The talk covered the range of indications including their efficacy for diabetes, cardiovascular disease, weight and obesity-related conditions and substance use disorder. Also, their anti-inflammatory effect (50% drops in CRP, even before weight loss), perhaps also on ageing – but limited data during pregnancy (currently not recommended) and in older people (especially >75 and any increased risk of fracture). All these are challenged by issues of access.
Lauren O’Connor from George Washington University presented a poster reporting use of GLP-1s among 13,000 participants in the observational DC Cohort Longitudinal HIV Study and in people who had had any prescription containing a GLP-1 or GLP-1/GIP. [2]
Overall, 578 participants included 82% with diabetes and 78% with obesity, 50% used semaglutide and median follow-up was three years. The mean BMI at baseline was 36.3 (SD +/– 8.1).
Overall, average weight loss was –2.5% with 31% losing >5% of weight and 11% losing >10%. The range of weight change was from –39% loss to +25% gain. Those who lost <10% were more likely to be non-Hispanic Black (p = 0.02) and have a history of diabetes (p<0.01). People without diabetes were more likely to report weight loss of >5% and >10%.
However, 71% of participants had at least one >3 month gap in treatment.
Two posters looked at the more recently approved GLP-1/GIP dual agonist tirzepatide – showing reductions in weight and HbA1c over 12 months, but without longer-term follow-up, especially concerning sustained access to this drug.
Heidi Crane from the University of Washington, Seattle, compared results of people starting tirzepatide (n=743) vs semaglutide from June 2022 to February 2025 at 9 clinic sites in the Centers for AIDS Research Network of Integrated Clinical Systems (CNICS) Cohort.
Baseline demographics included mean age 53 years, 28% were women, mean BMI was 35 kg/m2 (84% were >30) and 62% had diabetes.
Over 12 months, mean weight dropped by 5.9% (95% CI: –6.9 to –5.0) and mean HbA1c dropped by –0.58% (95% CI: –0.75 to –0.41). The only demographic difference was greater HbA1c decline in men –0.66% (95% CI: –0.87 to –0.46) compared to women –0.15% (95% CI: –0.23 to –0.07), p<0.01. These results were similar to semaglutide in adjusted analyses: weight –4.1% (95% CI: –4.6 to –3.5) and A1c –0.47% (95% CI: –0.58 to –0.36).
Lucas Hill from the University of California San Diego and colleagues reported limited short-term outcomes of tirzepatide in 61 people with HIV with and without diabetes that showed expected efficacy. [4]
Participants were largely white (52%), non-Hispanic (55%), male (67%) and taking oral INSTI-based ART (63%). Median BMI was 33 kg/m2 (IQR: 31 to 39) and comorbidities included hypertension (60%), high lipids (50%), diabetes (36%) and MASLD (27%).
Mean weight loss at months 3 (n=52), 6 (n=45), 9 (n=36) and 12 (n=34) was –7, –12, –12 and –15 kg respectively. Mean HbA1c decreased from 8% to 5.9% in the 12 people with diabetes who had data available. Mean systolic BP at 6 months dropped from 130.2 to 120.5 mmHg (n=47) p<0.001 and 26% (8/30) of those taking BP medication at baseline were able to reduce dosing.
However, 15 patients (25%) discontinued tirzepatide within 12 months due to side effects (n=6), access problems (n=8) or lack of efficacy (n=11).
Heidi Crane also presented a poster reporting that 204 people starting semaglutide significantly reduced the amount they smoked by 26%. This was the equivalent of smoking three less cigarettes a day (reduced from 10.5 to 7.8 (diff –2.7 (95% CI: –3.8 to –1.6), p<0.001. Importantly, 21% reported having stopped smoking at the follow-up visit. In adjusted analyses, similar results were reported independently of sex or BMI. [5]
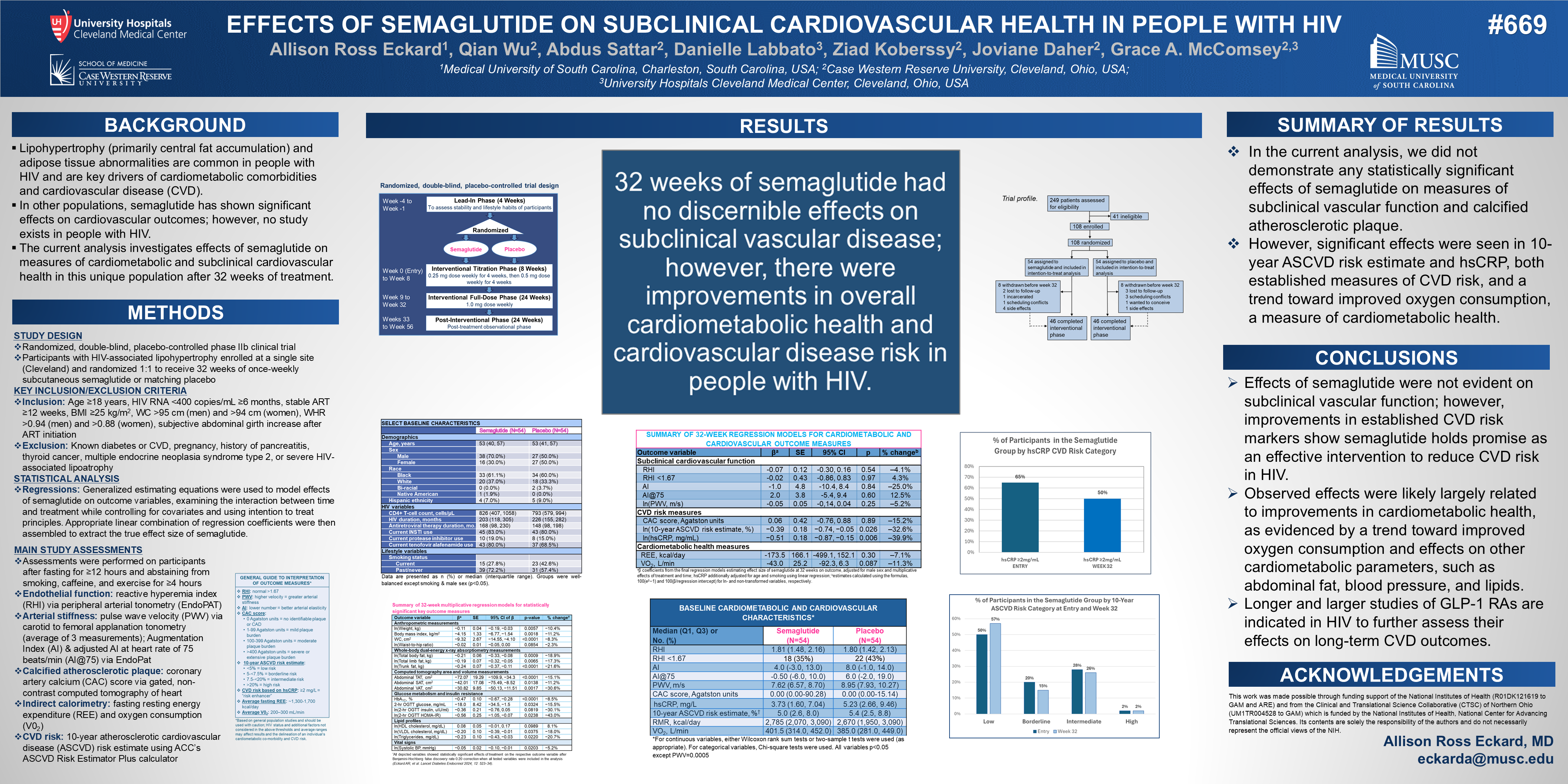
Allison Ross Eckard from the Medical University of South Carolina and colleagues presented results on subclinical cardiovascular health in 108 people on ART with BMI >25 kg/m2, without known diabetes, randomised (1:1) to semaglutide for 32 weeks or matching placebo. [6]
The study reported improvements in overall cardiometabolic health and cardiovascular disease risk with statistically significant decreases in the 10-year ASCVD risk score (ln β –0.39, CI –0.74, –0.05; p=0.026; % change –32.6%). However, there were no significant differences in arterial stiffness, endothelial function and calcified coronary atherosclerotic disease between the two groups, with researchers calling for larger studies.
Two other posters were presented from the CNICS study (see reference 3).
One looked and changes in depressive symptoms before and after starting semaglutide, presented by Lara Haidar from the University of Manitoba, Winnipeg. This study included 354 people starting semaglutide between 2018 and 2024 and depression was assessed using a 6-monthly PHQ-9 questionnaire. Median follow-up was 36 months before and 9 months after starting semaglutide.
Overall, no significant changes were reported (p=0.8). However, when analysed by baseline scores, those with lowest PHQ-9 (0 to 4) showed a small but significant increase after starting semaglutide (+1.2, p<0.001). Significant reductions were reported by people starting with progressively high baseline scores: –1.5, –2.8 and –4.7 in those with baseline scores of 5 to 9 (p=0.004), 10 to 14 (p=0.002) and >15 (p<0.001), respectively. [7]
The second reported on changes in liver fibrosis and metabolic dysfunction-associated steatotic liver disease (MASLD) in 1,850 people with longitudinal IB-4 scores before and after starting semaglutide. [8]
Overall at baseline, 1,467 (79%) had no/low fibrosis, 347 (19%) had moderate fibrosis, and 36 (2%) had advanced fibrosis. Most participants also had cardiometabolic conditions, drank low amounts of alcohol (57%) and did not have HCV (84%).
Although during a mean follow-up of 30 weeks on semaglutide there were no significant changes in the overall cohort, in subgroup analyses there were significant decreases in liver fibrosis score in participants with moderate-to-advanced fibrosis (change in FIB-4: 0.13, p<0.01) with the greatest decreases reported in those with advanced fibrosis at baseline (–1.05, p<0.001).
Finally, Miguel Marin from the Africa Health Research Institute in Durban reported on the gut-specific effects of liraglutide in a subgroup of five people who were either overweight or obese (median BMI 43 kg/m2), suppressed on ART and enrolled in the LIROH study. [9, 10]
This small uncontrolled study involved taking four sets of colonic and duodenal biopsies with matched blood samples at four timepoints: pre-treatment (T0), during 2-3 months on liraglutide and after 4 and 8 months washout (T2, T3). Results were compared to non-obese controls (median BMI=20) who were HIV– (n=13), HIV+ on ART (n=24) and HIV+ no ART (n=17).
As expected, high BMI and HbA1c at T0 both significantly reduced while on liraglutide at T1 and returned to baseline by T2 and T3. Significant reductions in the inflammatory marker hsCRP also dropped by T1 in some participants with drops in other plasma and tissue inflammatory mediators (exotaxin-3, IL-16, IL-12, IP-10 and I-FABP [Intestinal Fatty Acid Binding Protein – a marker of gut injury]). CD4 cells increased in the duodenum samples from 12% to 24% on treatment and reverted during washout. Median CD69 expression dropped from 74% at baseline to 13% on treatment and took longer to revert (25% at T2 and 54% at T3). PD-1 was up-regulated and CD8a receptor expression was down-regulated in gut T cells. These changes were not seen in plasma.
Spatial transcriptomics also indicated epithelial remodelling during liraglutide treatment. High-resolution spatial analysis showed GLP-1 absorption in and progressive reconstruction of microvilli architecture. This led the researchers to conclude that GLP-1 drugs might help repair gut damage that occurs during very early stages of HIV infection and persists even after years of suppressive ART.
The study also showed that people living with HIV and obesity have similar levels of inflammation on ART as HIV-positive people who are not obese and not on ART.
The tentative results from this small study report a new potential outcome from GLP-1 drugs that might reverse and potentially mitigate early gut damage.
The findings warrant further research, potentially using newer GLP-1 drugs.
comment
This is the third year that CROI has focussed on the limited data on GLP-1/GIP treatments in people living with HIV, even though they are now widely used, including in the UK, often through private prescription.
It is reassuring that these short-term studies show similar efficacy for people living with HIV to the general population. However longer follow-up is still very limited. People with HIV should not have been excluded from the phase 3 studies for these drugs and we shouldn’t have had to wait until semaglutide is virtually off-patent.
A very recent US study reported that 3 out of 4 people treated in the large Veteran’s Affairs database discontinued these drugs within the first 12 months, and the data gap for how to manage limited access will also be just as important for people living with HIV. Unfortunately, benefits of treatment tend to quickly reverse if treatment is stopped. [11]
Additional HIV-related data gaps include the impact of systemic fat loss on people who already have limited local fat due to lipoatrophy, especially on their face, legs or buttocks. One study reported this impact can worsen – and also reported the implications from loss of lean muscle that doesn’t naturally return when these drugs are discontinued – leading to a worse metabolic phenotype after short-term or intermittent use.
It is perhaps important for HIV doctors to now proactively ask the people in their care about use of and interest in GLP/GIP drugs. This would address any concerns about weight and body issues and help ensure HIV records include use of these meds if prescribed elsewhere, including via telehealth. It would also enable observational data for other effects of these drugs.
The potential to reduce substance use was also reported in the same US study – including nicotine, alcohol, cannabis, cocaine and other substances – and should also be actively studied in people living with HIV. [10]
The findings from the gut study are intriguing and warrant larger studies.
References
Unless stated otherwise, all references are to the Programme and Abstracts of CROI 2026, 22–24 February 2026.
www.retroconference.org
- Brown T. GLP-1 receptor agonists: Are they a cure for everything? CROI 2026, Denver. Oral abstract 24.
https://watch.croiwebcasts.org/2026croi/n/s/PL-02 (webcast) - O’Connor L et al. Evaluation of GLP-1 medications in an observational cohort of people with HIV in Washington DC. CROI 2026, Denver. Poster abstract 695.
https://www.croiconference.org/abstract/1293-2026 (abstract)
View e-poster (PDF) - Crane HM et al for the Centers for AIDS Research Network of Integrated Clinical Systems (CNICS) Cohort. Tirzepatide use in people with HIV shows effectiveness for weight loss and diabetes control. CROI 2026, Denver. Poster abstract 697.
https://www.croiconference.org/abstract/1266-2026 (abstract)
View e-poster. (PDF) - Hill L et al. Real-world outcomes of tirzepatide use in people with HIV with and without diabetes. CROI 2026, Denver. Poster abstract 696.
https://www.croiconference.org/abstract/1091-2026 (abstract)
View e-poster. (PDF) - Crane HM et al. Initiating semaglutide therapy reduces tobacco cigarette use among people with HIV. CROI 2026, Denver. Poster abstract 698.
https://www.croiconference.org/abstract/1308-2026 (abstract) - Ekhard AR et al. Effects of semaglutide on subclinical cardiovascular health in people with HIV. CROI 2026, Denver. Poster abstract 699.
https://www.croiconference.org/abstract/1826-2026 (abstract)
View e-poster (PDF) - Haidar L et al. The impact of semaglutide on depressive symptoms among people with HIV. CROI 2026, Denver. Poster abstract 447.
https://www.croiconference.org/abstract/1428-2026 (abstract)
View e-poster (PDF) - Ma J et al. Longitudinal Associations of Semaglutide With Liver Fibrosis Score in People With HIV. CROI 2026, Denver. Poster abstract 601.
https://www.croiconference.org/abstract/1785-2026 (abstract)
View e-poster. (PDF) - Marin M et al. GLP-1 RA Induces Gut T-Cell and Epithelial Remodeling in PWH From a Clinical Trial in South Africa. CROI 2026, Denver. Oral abstract 115.
https://watch.croiwebcasts.org/2026croi/ap/55037 (abstract) - ClinicalTrials.gov. LIROH – Liraglutide for Obesity in HIV (LIROH)
https://clinicaltrials.gov/study/NCT06438146 - GLP-1 receptor agonists reduce substance use disorder: a role for addiction to chemsex drugs? HTB (12 March 2026).
https://i-base.info/htb/53421
{kind=link}