
9.3 Mutations with and without drugs
9.3.1 Recap of previous section
The previous section started with important concepts.
- We have a genetic organism – in this case a virus (HIV).
- After infecting a CD4 cell, HIV can replicate many times. Every 1-2 days, in someone not on ART, HIV produces more than 100 million new virions.
- HIV has no proofreading mechanism. It makes at least one mistake (mutation) just by chance in each replication cycle.
- Someone who is not on ART is likely to have every possible single mutation. We don’t have one virus but a pool or soup of thousands of slightly different types of HIV.
9.3.2 Introduction to section 3
Section 3 looks at how HIV mutations behave when HIV drugs are around (i.e. in the presence of drugs).
9.3.3 Wild-type virus and drug pressure
In someone not on treatment, mutations that develop that can affect how a drug works are made at random.
When HIV contains no dominant drug resistant mutations, this is called ‘wild-type’ virus.
Mutations generally make HIV less fit at replicating. Wild-type HIV is therefore stronger and fitter that drug resistant HIV.
When not on ART, mutations that are drug resistant have no advantage over wild-type HIV. These mutations are less fit and so wild-type continues to be dominant. The mutation may still be in the pool of viruses but it will stay a minority.
- The main strain will be the fittest virus (ie wild-type when not on treatment).
- A mutation that stops a drug working is called ‘a mutation associated with drug resistance’ or, more commonly, ‘a drug resistant mutation’.
- As long as you are not taking the drug associated with this resistance, this mutation will have no relative advantage over wild-type virus.
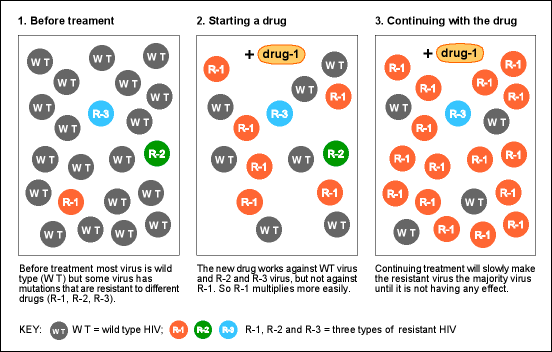
Now think about how the pool of viruses will change if you start taking this drug.
- The drug will be able to kill most of the viruses in the pool. However, it will not be active against the virus that is resistant to the drug.
- The drug resistant virus will continue to replicate. This resistant virus now has an advantage over the other viruses. It is relatively more fit.
- Slowly, the drug resistant HIV will become dominant.
- In the presence of the drug, further mutations can develop and make the resistance even stronger.
Before taking ART the resistant HIV had no advantage over wild-type. Now, it is stronger than the other viruses. See Figure 2.
This major concept is called ‘survival of the fittest’. In biology, this is the concept that explains evolutions of life from amoeba to humans.
Figure 2: How resistant mutations respond to treatment
9.3.4 Survival of the fittest
‘Survival of the fittest’ is central to the concept of evolution.
Whether talking about how life developed from tiny organisms into plants, fish, birds, animals and humans, or how a virus changes, life evolves. It has taken millions of years for humans to evolve, but HIV does this in days.
Each generation evolves and adapts in relation to the surrounding environment.
This is the same for HIV. The virus evolves and when the environment changes this affects how HIV evolves. By taking treatment, the environment for the virus changes because the virus is now in the presence of drugs.
This idea is sometimes explained another way. Treatment is referred to as exerting a selective pressure on the virus to change.
- This pressure is encouraging the resistant virus to reproduce.
- It is a selective pressure, because it is encouraging the mutations linked to resistance to that drug to be selected over those without resistance.
9.3.5 Selective pressure
Sections 3.1 to 3.4 involved important ideas. If you want to, take a break to let these ideas sink in.
These ideas will be the foundations for the next sections, which should be easier. Take time to recap the following key points.
Key point 1: HIV drugs do not initially cause resistance. Mutations occur because the virus makes mistakes. However, a drug exerts selective pressure for resistance to develop and expand.
Although the first mutations occur by chance, often before ART, if HIV continues to replicate in the presence of ART, this can generate new and more complicated patterns of resistant mutations.
The second and third mutations would not be likely to occur naturally if the treatment wasn’t present. This means that if you stay on a failing treatment then more complicated mutations can occur.
Key point 2: is that selective pressure of drugs can work in two ways.
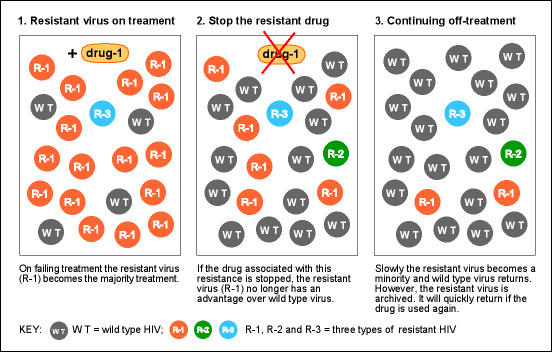
If you stop or switch treatment then the drug pressure is taken away. This will reduce the amount of resistant virus in the pool. Without the drug, the resistant HIV no longer has a relative advantage over wild-type.
- Wild-type virus is better at replicating than resistant HIV, when there are no drugs.
- When the drug pressure is removed, wild-type HIV then becomes the majority virus.
- The time this takes depends on the specific mutation. Mutations that develop easily are sometimes the fastest to reduce when a drug is stopped.
Question: Does drug resistance disappear when you stop taking a drug?
Answer: No. Drug resistant HIV becomes a minority in the pool (see Figure 3) and is archived in CD4 cells that are sleeping. Sometimes this can happen within weeks and sometimes it might take years.The resistant HIV then becomes too difficult to detect with a standard resistance test. Also see Section 5: When to use resistance tests.
Figure 3: Resistance reduces if treatment is stopped but it remains at low levels
Key point 3: A resistance test only tells you about resistance to the drugs that were being taken when the blood sample was taken. When looking for transmitted drug resistance, the sample closest to the time of infection is most likely to still see resistance.
This point is important when advocating for resistance testing.
If you are infected with drug resistant HIV, this will initially be your dominant strain. Over time, some mutations become a minority at a level that is too low to be detected. Even though the majority population may become wild type HIV, drug resistance will still be present. This is called ‘archived resistance’.
- UK guidelines recommend resistance testing for everyone who is newly diagnosed with HIV.
- If a resistance test is not provided, a blood sample needs to be taken and stored. This is so it can be tested before starting treatment.
- UK guidelines also recommend resistance testing when viral load has rebounded on treatment and when treatment has never reduced viral load to undetectable.
Key point 4: Drug resistant HIV can be transmitted in the same ways as wild-type HIV. This includes sexually, through shared injecting equipment, from needle-stick injuries and from mother to baby. If is also possible for people who are already HIV positive to be reinfected with a different drug resistant strain.
Many cases of re-infection are only detected because the new infection was with drug-resistant HIV.
About 10% of new infections in the UK are with HIV that has at least one major mutations to at lest one drug. A smaller percentage has HIV that is resistant to two or more drugs. Although rare, some people are infected with HIV that is resistant to three or more drugs or drug classes. (See this case of transmission of five class resistance.)
- The longer the time from infection to diagnosis, the more difficult it is to detect some types of transmitted resistance.
- Some mutations drop below the levels that can be detected by resistance tests within a few months but some mutations can still be detected after several years.
Question: What happens if someone was infected with HIV that was drug resistant and starts treatment that includes one of those drugs?
Answer: If they are using a combination with three drugs, then only two of those drugs will be fully active. This increases the risk that the combination may not be strong enough. It will be more difficult to get an undetectable viral load and resistance to the other drugs can develop.
9.3.6 Using three drugs in HIV treatment
The example in Figure 2 shows that using a single drug provides pressure for pre-existing resistance to become dominant.
This is one reason why combination therapy uses three drugs. See Figure 4.
Single mutations are all present when starting ART. Some dual resistant mutations may be present on a few viruses. But triple resistance will not be present on the same viruses. Even with HIV being such a rapid and prolific virus, this is very unlikely.
Figure 4: Combinations with three drugs work against low-level pre-existing resistance

In Figure 4, virus R-1 is resistant to Drug-1, R-2 is resistant to D-2 and R-3 is resistant to D-3. Although R-1, R-2 and R-3 mutations are all present when starting treatment, these three different mutations are very unlikely to have all developed on the same virus.
HIV that is already resistant to Drug-1, will be killed by D-2 and D3. The virus resistant to Drug-2 will be killed by D-1 and D3.
Even if R-1 and R-2 have developed on the same virus (dual resistance) then D-3 will still be active against this virus.
D-1, D-2 and D-3 will also all be active against wild-type HIV, which is hopefully the majority population.
9.3.7 Section 3: Learning points
- HIV drugs do not initially cause resistance. Mutations occur because HIV makes mistakes and there is no proofreading mechanism.
- A drug exerts selective pressure for resistance to develop.
- Under continued drug pressure, more complicated patterns of resistance mutations develop that only occur because of this continued drug pressure.
- Results from resistance tests only accurately tell you about resistance to the drugs that were being taken when the blood sample was drawn.
- Without drugs, wild type virus is more fit than resistant virus.
- Drug resistant HIV can be transmitted in all the same ways the wild type virus can be transmitted. See section 6.5.
- Someone can be infected by a virus that is already resistant to one or more drugs.
- An HIV positive person can be reinfected with a different strain of HIV. Cases of reinfection are only usually detected when the new infection (or superinfection) is with drug-resistant HIV. See section 6.8.
- Reinfection with drug resistant HIV can have serious health implications because there are fewer drugs to choose from.
- Combination therapy uses three active drugs to try to ensure it is active against pre-existing resistance.
9.3.8 Section 3 evaluation
Please take a few minutes to evaluate this session online.
This single page includes six short questions.
Your answers are anonymous, but the course is dependent on your feedback, which is appreciated.
Last updated: 1 January 2023.